Contribution of anxiety and dialysis factors to the event of fatigue in hemodialysis patient
Yanti Cahyati, Ida Rosdiana
Poltekkes Kemenkes Tasikmalaya. Indonesia. Health and Disaster Emergency (HADE) Center. Center of Excellence. Poltekkes Kemenkes Tasikmalaya. Indonesia
https://doi.org/10.37551/52254-28842022017
Como citar este artículo:
Yanti C, Ida R. Contribution of anxiety and dialysis factors to the event of fatigue in hemodialysis patient.
Enferm Nefrol. 2022;25(2):156-61
Correspondencia:
|
Recepción: 22-06-2021
|
ABSTRACT
Introduction: Fatigue is one of the most common symptoms felt by chronic renal failure patients undergoing hemodialysis (HD). The prevalence ranges from 42-97% with levels varying from low to severe. Fatigue is not only detrimental to physical and social functioning but is also associated with poor quality of life for HD patients and is associated with death in patients undergoing chronic hemodialysis. For this reason, it is necessary to know the factors associated with the incidence of fatigue so that appropriate interventions can be carried out, both pharmacologically and non-pharmacologically.
Objective: To evaluate the influence of anxiety and dialysis factors on the incidence of fatigue in patients undergoing hemodialysis at Ciamis Hospital.
Material and Method: A cross sectional approach with a total sample of 88 people was used.
Results: The results showed that 78 respondents (88.6%) who experienced fatigue complaints and anxiety had a relationship with the incidence of fatigue (OR: 9.0; p=0.019).
Conclusions: Psychological factors, such as anxiety, are associated with the fatigue experienced by patients on hemodialysis.
Keywords: hemodialysis; fatigue; dialysis; psychological.
RESUMEN
Influencia de la ansiedad y de los factores de la diálisis en el desarrollo de fatiga en el paciente hemodializado
Introducción: La fatiga es uno de los síntomas más comunes en los pacientes con enfermedad renal crónica en hemodiálisis (HD). La prevalencia oscila entre 42 y 97% de incidencia con niveles de intensidad variables desde leve a severa. La fatiga no es solo perjudicial para el desempeño físico y social del paciente pues además está asociada a una baja calidad de vida de los pacientes en hemodiálisis. Por esta razón, es necesario conocer los factores asociados a la incidencia de fatiga para que puedan llevarse a cabo las intervenciones adecuadas, sean farmacológicas o no.
Objetivo: Evaluar la influencia de factores relacionados a ansiedad y diálisis en la incidencia de fatiga en pacientes de diálisis en el Hospital Ciamis.
Material y Método: Se llevó a cabo un estudio transversal en una muestra de 88 pacientes.
Resultados: Setenta y ocho pacientes (88,6%) con fatiga declaraban que la ansiedad tiene una relación con la incidencia de la fatiga (OR:9,0; p=0,019).
Conclusiones: Factores psicológicos como la ansiedad están asociados a la aparición de fatiga en pacientes en hemodiálisis.
Palabras clave: hemodiálisis; fatiga; diálisis; psicológico.
INTRODUCTION
Chronic kidney disease is a severe health problem that needs to be addressed more effectively. The higher the rate of chronic kidney disease events, the more consistent with the increased cost of hemodialysis therapy that must be undergone for the lifetime of chronic kidney disease patients. Chronic kidney disease treatment is the second-most-financialized health service, after heart illness. This, of course, will result in rising health costs and reduced living quality for patients with chronic kidney diseases1. One of the complications that are often experienced by chronic renal failure patients undergoing hemodialysis is fatigue2-3.
Fatigue is defined as feeling extremely tired at rest, fatigue with activity, lack of energy that hinders daily tasks, inertia or lack of endurance, and loss of enthusiasm4. Horigan et al. (2006)5 defined fatigue as a subjective state of exhaustion that is experienced as an unpleasant and difficult life experience. The prevalence of fatigue in various studies varies widely due to differences in definitions, diagnosis, population characteristics, and research methodologies. Fatigue is at least 42-97% of patients undergoing hemodialysis6-7.
The consequences of fatigue experienced by hemodialysis patients include decreased motivation, disruption of social relationships, decreased quality of sleep, and increased pain, which can reduce the quality of life of patients6,8-9. Fatigue is also proven to be associated with the patient’s clinical condition and increases the risk of cardiovascular disease and death, so it is necessary to carry out proper management according to the factors that influence it5,6,8,10.
Various factors that are thought to have a significant relationship with the occurrence of fatigue in hemodialysis patients are demographic factors3,9,11,12, physiological factors/clinical factors13,14 psychological factors6,15, and therapy/dialysis factors12,16. Fatigue experienced by hemodialysis patients is one of the nursing problems that need to be handled accurately because it requires the role of nurses who can overcome it through comprehensive nursing care. The goal is to improve the quality of life of patients and reduce complications arising from fatigue experienced by hemodialysis patients. Nurses’ understanding of the fatigue experienced by dialysis patients is an important part of providing effective nursing care. This study aims to identify the influence of anxiety and dialysis factors on the incidence of fatigue in hemodialysis patients.
MATERIAL AND METHOD
Study Design
The research design used a cross sectional approach.
Participants and Sample Selection Process
Of the 110 patients that make up the usual population of the Ciamis General Hospital, only 88 of them met the inclusion criteria of the study. The inclusion criteria for this research sample were: compos mentis awareness and ability to communicate naturally, can read and write, willing to be respondents. The sample exclusion criteria were experiencing motoric, sensory and global aphasia and experiencing intradialytic complications.
Data Collection
The study was conducted in the hemodialysis room of the Ciamis General Hospital from October to November 2020. The timing of data collection was suited to the respondent’s hemodialysis schedule, and using a questionnaire. A questionnaire was used to collect data in this study, that included questions about demographics data, dialysis factors, anxiety, and fatigue. Data collection begins with determining respondents who meet the inclusion criteria according to the sampling technique, asking the respondent’s willingness to become a sample by first explaining the aims and objectives of the research, voluntarily asking the respondent to sign a sheet of informed consent, and asking them to fill out a questionnaire that has been prepared. Observations were made to monitor the patient’s physical health condition.
Assessment of Fatigue and Anxiety
Assessment of patient fatigue was carried out using the Visual Analog Scale (VAS-F). Traditionally, the visual analog scale (VAS) consisted of a 10 cm horizontal line with a written description at each end17. In this study, respondents were asked to mark on a dotted line which they felt represented their perception of their current state of fatigue. Possible scores range from 0 to 10 circled by the respondent using a pen. The score was obtained by measuring the line from “No Fatigue” to the point indicated by the subject representing his or her level of fatigue. The higher the VAFS score, the higher the fatigue. In this study, respondents who circled the number 0-4 were declared not to be fatigued, while those who circled the number 5-10 were stated to be experiencing fatigue18,19.
Anxiety in this study is defined as the respondent’s psychological response to the problem/disease being faced, categorized into mild anxiety and severe anxiety. Anxiety assessment was carried out using the Taylor Manifest Anxiety Scale (TMAS) which consisted of 24 questions. The score for positive statements is one (1), while for negative statements zero (0). The results of the measurement of the level of anxiety are categorized in the form of ratio data with a value of 0-24, then categorized into two categories, namely mild anxiety if the number of answer scores is below the value mean (<12), and severe anxiety if the number of answer scores is above or equal to the mean (≥12). The cutoff point for these two categories is the mean value because the data is normally distributed.
Validity and reliability tests were carried out at the Banjar Hospital. Analysis of validity and reliability tests using computer software with degrees of freedom 30-2=28 (r table 0.361). The validity of the anxiety questionnaire test was declared valid because all questions had an r arithmetic value greater than the r table. The result of the reliability test is Cronbach’s r alpha 0.915 (r alpha>0.361), so the questionnaire is reliable20.
Statistical Analysis
Statistical analysis was performed with IBM SPSS software vs.20. A descriptive analysis was performed for the quantitative variables: age (mean and standard deviation), for the qualitative variables, measures of frequencies and percentages were calculated. For the analysis of the variables, the test Chi-Square which was used to test the hypothesis of a significant relationship between anxiety and dialysis factors with the incidence of fatigue. Values of p<0.05 were considered statistically significant.
Ethical Principles
Informed consent on patients, who guarantee their willingness to participate in research and informed confidentiality. The personal information obtained is guaranteed confidentiality and is used only for research purposes. The research adheres to ethical standards as well as current international data protection requirements and Indonesian legislation. Ethical approval gets from the Research Ethics Commission for STIKES Ahmad Yani Cimahi No.002/KEPK/X/2020. The authors declare not to have any interest conflicts.
RESULTS
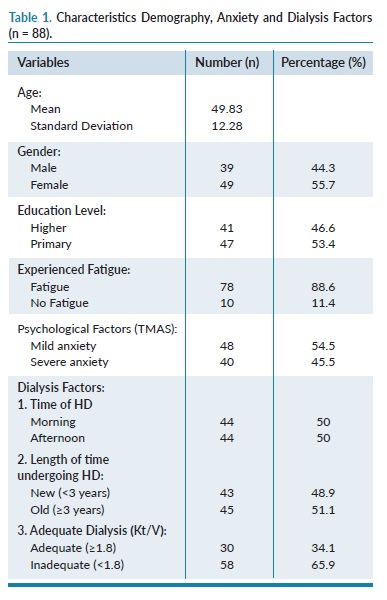
The results of this study showed that the mean age of respondents was 49.83 years (±12.28), 55.7% were female, 53.45% of respondents were education level is primary, 88.6% of respondents were experienced fatigue, 54.5% were mild anxiety. Base on dialysis factors, 50% respondents were ongoing hemodialysis at morning and 50% at afternoon, 51.11% respondents have hemodialysis >3 years, 65.9% respondents have Kt/V<1.8 (inadequate) (table 1).
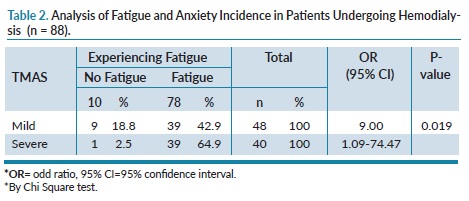
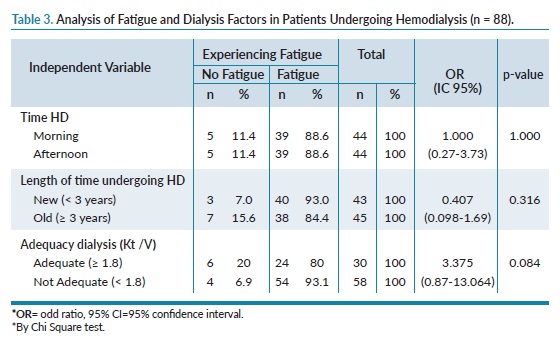
The results of the analysis show that there is a significant difference in the proportion of fatigue events in respondents who experience mild anxiety and severe anxiety, the odds ratio (OR)=9.00 (95% CI), means that respondents who experience severe anxiety have 9 times the opportunity to experience fatigue compared to respondents who experience mild anxiety (table 2). There is no relationship between Time of HD, time spent undergoing HD, and dialysis adequacy (Kt / V) with the incidence of fatigue (table 3).
DISCUSSION
Several studies have reported a high incidence of fatigue in patients undergoing hemodialysis10.16,11,21. The results of this study also found that the incidence of fatigue in patients undergoing hemodialysis was quite high, namely 88.6% of 88 respondents. This number is higher when compared with the results of previous studies3,22. The high incidence of fatigue in this study is probably related to the high number of respondents who experience psychological problems (anxiety), where this condition is reported to have a significant relationship with the incidence of fatigue6. Several studies have shown a significant relationship between psychological factors and fatigue in HD patients. Patients who experience psychological problems such as anxiety, depression, and stress experience higher levels of fatigue6. Chilcot et al15 concluded that mood and beliefs are associated with fatigue in HD patients.
Fatigue in uremic patients has greater consequences than in the general population. Fatigue in HD patients not only impairs physical and social functioning but is also associated with poor quality of life and premature death in HD patients7. Research Marit S et al23, shows that anxiety and depression are closely related to the fatigue experienced by patients undergoing HD. Conditions of anxiety, depression, and fatigue are the causes of decreased quality of life for HD patients. It was found that anxiety scores were increasing in HD patients who experienced fatigue. This study also concluded that the determinant factor that affects the quality of life of HD patients, one of that is anxiety that often experienced by HD patients who experience fatigue.
Another study states that HD patients generally experience severe fatigue24,25. These patients’ mean vitality scores were lower than for most other chronic health conditions. More than 50% of the patients in this study had poor vitality scores out of 50, which is comparable to those with major depression, cancer patients undergoing chemotherapy, and people with lupus. This shows how important this fatal incident can be identified so that it can improve the quality of life for HD patients25.
The results of the study by Sulistini, Yetty, Hariyati26, regarding the factors that influence fatigue in HD patients found that there was no relationship between situational factors consisting of frequency, HD complications, and disease history with the incidence of fatigue, but it was found that there was a relationship between the length of undergoing HD. with complaints of fatigue in HD patients. This is different from what the researchers found, where the length of time undergoing HD was not correlated with the incidence of fatigue. Based on the results of Maesaroh research (2020)26, it was found that respondents did hemodialysis is mostly more than 5 years.
Research conducted (Krishan et al, 2014)26 stated that fatigue began to be experienced by patients undergoing dialysis on average the first 6 to 8 months and fatigue will decrease at the end of dialysis visits. Severe fatigue experienced in the first month of undergoing hemodialysis. Fatigue was very severe experienced in the first six months undergoing hemodialysis. The results of these studies illustrate that in the initial phase of undergoing hemodialysis patients experience increased fatigue. This means that the longer the patient undergoes hemodialysis, the level will decrease fatigue because it has undergone an adjustment phase.
Previous studies have shown that the relationship between dialysis adequacy and fatigue is inconsistent. In this study, Kt/V was used to measure the level of dialysis adequacy with a minimum number of 1.8. The study results showed that 65.9% of respondents had inadequate dialysis and further analysis showed that there was no relationship between dialysis adequacy and fatigue (p-value 0.084). These results are in line with the research of Maesaroh, et al (2020)25 but contradict the research of Dadgari, et al (2015)27. Adequate dialysis is a term used for many years based on small solute clearance measurements using urea and creatinine. Adequate dialysis aims to slow down the death process, prolong life and improve the quality of life of patients undergoing hemodialysis28. The Ministry of Health of the Republic of Indonesia recommends adequate dialysis with a URR value of 80%. The standard Kt/V value is 1.2 for patients three times a week and 1.8 for patients twice a week29.
The main limitation of this research is the existence of several variables that were not examined. Researchers only studied the relationship between anxiety and fatigue in HD patients, in the psychological aspect. In contrast, other psychological problems should be investigated, such as depression and decreased quality of life.
This study conclude that anxiety and fatigue are associated in hemodialysis patients. The results of this study provide recommendations on the importance of identifying complaints of fatigue, especially in patients who have just undergone HD, so that appropriate and rapid intervention can be done to improve the quality of life of patients with kidney failure.
ACKNOWLEDGEMENTS
The author expressed thankfulness to all those who participated in the research, including nurses from Ciamis General Hospitals, all hemodialysis patients in Ciamis General Hospital, and all those who supported until the publication of this article.
Conflict of interest:
The authors declare that they have no potential conflicts of interest related to the contents of the article.
BIBLIOGRAFÍA
1. Kallenbach JZ. Review of hemodialysis for nurses and dialysis personnel-e-book. Elsevier health sciences; 2020.
2. Jeon HO, Kim J, Kim O. Factors affecting depressive symptoms in employed hemodialysis patients with chronic renal failure. Psychol Heal Med;25(8):940-9.
3. Zyga S, Alikari V, Sachlas A, Fradelos EC, Stathoulis J, Panoutsopoulos G, et al. Assessment of fatigue in end stage renal disease patients undergoing hemodialysis: prevalence and associated factors. Med Arch. 2015;69(6): 376-80.
4. Davis MP, Walsh D. Mechanisms of fatigue. J Support Oncol 2010;8(4):164–74.
5. Horigan AE. Fatigue in hemodialysis patients: a review of current knowledge. J Pain Symptom Manage. 2012;44(5):715–24.
6. Picariello F, Moss-Morris R, Macdougall IC, Chilcot J. The role of psychological factors in fatigue among end-stage kidney disease patients: a critical review. Clin Kidney J. 2016;10(1):79–88.
7. Jhamb M, Abdel-Kader K, Yabes J, Wang Y, Weisbord SD, et al. Comparison of Fatigue, Pain, and Depression in Patients With Advanced Kidney Disease and Cancer—Symptom Burden and Clusters. J Pain Symptom Manage. 2019;57(3):566–75.
8. Chiaranai C. The lived experience of patients receiving hemodialysis treatment for end-stage renal disease: a qualitative study. J Nurs Res. 2016;24(2):101–8.
9. Strippoli GF, Craig JC, Tong A, Saglimbene VM, Unruh ML, et al. Interventions for fatigue in people with chronic kidney disease requiring dialysis. Cochrane Database Syst Rev. 2018(8).
10. Letchmi S, Das S, Halim H, Zakariah FA, Hassan H, Mat S, et al. Fatigue experienced by patients receiving maintenance dialysis in hemodialysis units. Nurs Health Sci. 2011;13(1):60–4.
11. Jhamb M, Weisbord SD, Steel JL, Unruh M. Fatigue in patients receiving maintenance dialysis: a review of definitions, measures, and contributing factors. Am J Kidney Dis. 2008;52(2):353-65.
12. Sajadi A, Farahani B, Zanjani E, Durmanesh B, Zare M. Factors affecting fatigue in chronic renal failure patients treated with hemodialysis. Iran J Crit Care Nurs. 2010;3:33-8.
13. Johansen KL, Finkelstein FO, Revicki DA, Evans C, Wan S, Gitlin M, et al. Systematic review of the impact of erythropoiesis-stimulating agents on fatigue in dialysis patients. Nephrol Dial Transplant. 2011;27(6):2418-25.
14. Yamasaki A, Yoda K, Koyama H, Yamada S, Tsujimoto Y, Okuno S, et al. Association of erythropoietin resistance with fatigue in hemodialysis patients: a cross-sectional study. Nephron. 2016;134(2):95-102.
15. Chilcot J, Norton S, Kelly ME, Moss-Morris R. The Chalder Fatigue Questionnaire is a valid and reliable measure of perceived fatigue severity in multiple sclerosis. Mult Scler J. 2016;22(5):677-84.
16. Biniaz V, Tayybi A. Nemati E, Shermeh MS, Ebadi A. Different aspects of fatigue experienced by patients receiving maintenance dialysis in hemodialysis units. Nephrourol Mon. 2013;5(4):897-900.
17. Wewers ME LN. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Heal. 1990;13(4):227–36.
18. Auliasari BM, Maliya A, Kesehatan. Pengaruh Aromaterapi Terhadap Tingkat Kelelahan (Fatigue) pada Pasien Gagal Ginjal yang Menjalani Terapi Hemodialisa. Semin Nas Keperawatan Univ Muhammadiyah Surakarta. 2020;45–53.
19. Faizal M, Nur BM, Rayasari F, Citra S, Belitung DB. Management Self Care Fatigue Klien End Stage Renal Disease Yang Menjalankan Hemodialisa. J Keperawatan Pangkalpinang. 2018;1(1):28–35.
20. Rosdiana I, Yetty K, Sabri L. Kecemasan dan lamanya waktu menjalani hemodialisis berhubungan dengan kejadian insomnia pada pasien gagal ginjal kronik. J Keperawatan Indonesia. 2014;17(2):39–47.
21. McCann K, Boore JRP. Fatigue in persons with renal failure who require maintenance haemodialysis. J Adv Nurs. 2000;32(5):1132–42.
22. Bossola M, Di Stasio E, Antocicco M, Pepe G, Marzetti E, Vulpio C. 1-year course of fatigue in patients on chronic hemodialysis. Int Urol Nephrol. 2017;49(4); 727-34.
23. Sandwijk MS Van, Arashi D Al, Bijlsma JA, Bemelman FJ. Fatigue, anxiety, depression and quality of life in kidney transplant recipients,haemodialysis patients, patients with a haematological malignancy and healthy controls. 2018;833–8.
24. Jhamb M, Weisbord SD, Steel JL, Unruh M. Dialysis: A Review of Definitions, Measures, and Contributing Factors. Am J kidney Dis. 2008;52(2):353–65.
25. Maesaroh, Agung Waluyo WJ. Faktor-Faktor yang Berhubungan dengan Terjadinya Fatigue pada Pasien Hemodialisis. Jurnal Ilmiah Indonesia. 2020;5(4):110–20.
26. Sulistini R, Yetti, Krisna, Hariyati T. Faktor faktor yang mempengaruhi Fatique pada Pasien yang Menjalani Hemodialisa. J Keperawatan. 2012;15(2):75–82.
27. Dadgari A, Dadvar L, Eslam-Arrow H. Multidimensional fatigue syndrome and dialysis adequacy among elderly patients under hemodialysis treatment. International Journal of Health Studies. 2015;2(1):5–8.
28. Dehvan F, Monjazebi F, Khanghahi ME, Mohammadi H, Ghanei Gheshlagh R, Kurdi A. Adequacy of dialysis in Iranian patients undergoing hemodialysis: A systematic review and meta-analysis. Nephrourol Mon. 2018;10(5); 1-10.
29. Indonesia Renal Registry. IRR. 10th report of Indonesian renal registry. Sekretariat Registrasi Ginjal Indonesia. 2014.
Este artículo se distribuye bajo una Licencia Creative Commons Atribución–NoComercial 4.0 Internacional.
https://creativecommons.org/licenses/by-nc/4.0/
